Fillable Immunization Record Template
File Details
| Fact Name | Details |
|---|---|
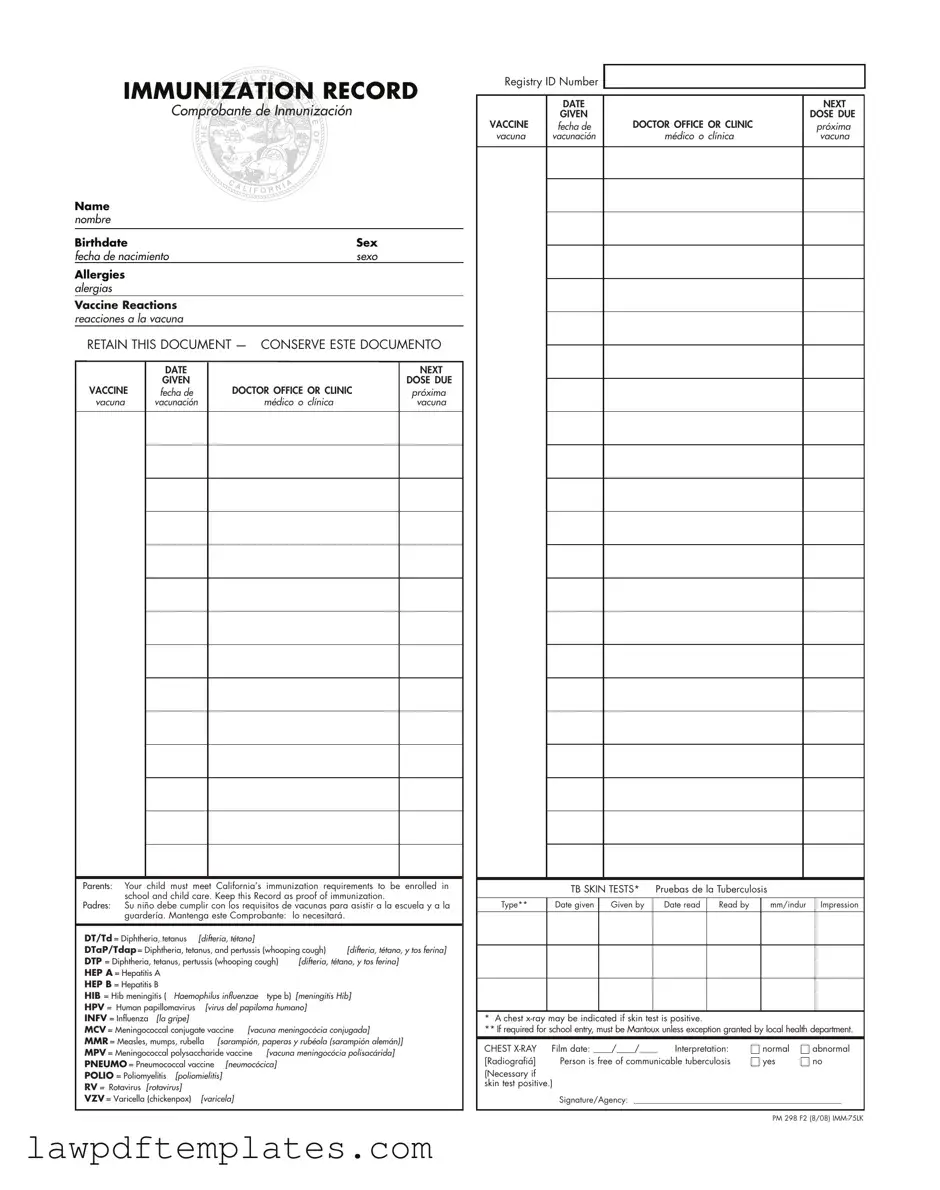
| Purpose of the Form | The Immunization Record form serves as proof of a child's vaccinations, which is necessary for enrollment in schools and child care facilities in California. |
| Required Information | This form must include the child's name, birthdate, sex, allergies, vaccine reactions, and details about each vaccine administered, including the date given and the next dose due. |
| Legal Requirements | California law mandates that children must meet specific immunization requirements to attend school and child care. These laws are outlined in the California Health and Safety Code. |
| Retention of the Document | Parents are advised to keep this document as it is essential for school enrollment and may be required for future medical needs. |
Sample - Immunization Record Form
IMMUNIZATION RECORD
Comprobante de Inmunización
Name nombre
Birthdate |
|
|
Sex |
||
fecha de nacimiento |
|
sexo |
|||
Allergies |
|
|
|
|
|
alergias |
|
|
|
|
|
Vaccine Reactions |
|
|
|
|
|
reacciones a la vacuna |
|
|
|
|
|
RETAIN THIS DOCUMENT — CONSERVE ESTE DOCUMENTO |
|||||
|
DATE |
|
|
NEXT |
|
|
|
|
|||
|
GIVEN |
|
|
DOSE DUE |
|
VACCINE |
fecha de |
DOCTOR OFFICE OR CLINIC |
|
próxima |
|
vacuna |
vacunación |
médico o clínica |
|
vacuna |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Parents: Your child must meet California’s immunization requirements to be enrolled in school and child care. Keep this Record as proof of immunization.
Padres: Su niño debe cumplir con los requisitos de vacunas para asistir a la escuela y a la guardería. Mantenga este Comprobante: lo necesitará.
DT/Td = Diphtheria, tetanus |
[difteria, tétano] |
|
|
|
|
DTaP/Tdap = Diphtheria, tetanus, and pertussis (whooping cough) |
[difteria, tétano, y tos ferina] |
||||
DTP = Diphtheria, tetanus, pertussis (whooping cough) |
[difteria, tétano, y tos ferina] |
||||
HEP A = Hepatitis A |
|
|
|
|
|
HEP B = Hepatitis B |
|
|
|
|
|
HIB = Hib meningitis ( |
Haemophilus influenzae |
type b) |
[meningitis Hib] |
||
HPV = Human papillomavirus |
[virus del papiloma humano] |
|
|||
INFV = Influenza [la gripe] |
|
|
|
|
|
MCV = Meningococcal conjugate vaccine [vacuna meningocócia conjugada] |
|||||
MMR = Measles, mumps, rubella [sarampión, paperas y rubéola (sarampión alemán)] |
|||||
MPV = Meningococcal polysaccharide vaccine |
[vacuna meningocócia polisacárida] |
||||
PNEUMO = Pneumococcal vaccine [neumocócica] |
|
|
|||
POLIO = Poliomyelitis |
[poliomielitis] |
|
|
|
|
RV = Rotavirus [rotavirus] |
|
|
|
|
|
VZV = Varicella (chickenpox) |
[varicela] |
|
|
|
|
Registry ID Number
|
DATE |
|
NEXT |
|
GIVEN |
|
DOSE DUE |
VACCINE |
fecha de |
DOCTOR OFFICE OR CLINIC |
próxima |
vacuna |
vacunación |
médico o clínica |
vacuna |
|
TB SKIN TESTS* |
Pruebas de la Tuberculosis |
|
|
|||
|
|
|
|
|
|
|
|
Type** |
Date given |
Given by |
Date read |
Read by |
|
mm/indur |
Impression |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
* A chest
** If required for school entry, must be Mantoux unless exception granted by local health department.
CHEST |
Film date: ____/____/____ |
Interpretation: |
|
normal |
|
abnormal |
|
[Radiografiá] |
Person is free of communicable tuberculosis |
|
yes |
|
|
no |
|
|
|
|
|||||
(Necessary if skin test positive.)
Signature/Agency: __________________________________________________
PM 298 F2 (8/08)
Common mistakes
Filling out the Immunization Record form can seem straightforward, but many people make common mistakes that can lead to complications. One frequent error is not providing complete information in the Name section. Omitting a middle name or using nicknames can create confusion. Always use the full legal name as it appears on official documents.
Another mistake occurs when individuals fail to include the correct Birthdate. An incorrect birthdate can delay school enrollment or other important processes. Double-check the date to ensure accuracy. Additionally, some may overlook the Sex field. This information is vital for proper record-keeping and immunization tracking.
People often neglect to list any Allergies their child may have. This omission can be crucial, especially if a vaccine contains ingredients that could trigger an allergic reaction. Always provide a complete list of known allergies to avoid potential health risks.
When it comes to documenting Vaccine Reactions, many forget to include this important information. If a child has had adverse reactions to previous vaccinations, this should be noted on the form. This helps healthcare providers make informed decisions about future immunizations.
Another common error is failing to retain the document as instructed. Many parents do not keep a copy of the Immunization Record, which can lead to problems later on. This document serves as proof of immunization, and losing it can complicate school enrollment.
Some individuals might also forget to fill in the Registry ID Number. This number is essential for tracking immunization records within the healthcare system. Ensure this field is completed to facilitate any necessary follow-up.
People sometimes misinterpret the DATE NEXT GIVEN section. This date should reflect when the next dose is due, not when it was last administered. Accurate tracking of vaccination schedules is crucial for maintaining proper immunization.
Lastly, many overlook the importance of the Signature/Agency section. This part confirms that a qualified individual has reviewed the immunization information. Failing to include a signature can render the form incomplete, leading to delays or rejections.
Common PDF Documents
Free Printable 5 Wishes Form - Five Wishes invites individuals to consider their own comfort and treatment preferences during serious illness.
I-589 Application - Filing the I-589 can also lead to the possibility of obtaining a green card.
A Colorado Do Not Resuscitate (DNR) Order form is a legal document that allows individuals to refuse resuscitation efforts in the event of a medical emergency. This form ensures that a person's wishes regarding life-sustaining treatment are respected by healthcare providers. For those interested in preparing this important document, the Do Not Resuscitate Order form provides essential guidance on how to properly complete and utilize it, making it crucial for anyone considering their end-of-life care options.
How to Get Acord Insurance Certificate - The Acord 50 WM form supports effective record-keeping practices.