Fillable DD 2870 Template
File Details
| Fact Name | Description |
|---|---|
| Purpose | The DD Form 2870 is used to authorize the release of medical information from military health care providers. |
| Eligibility | Active duty service members, veterans, and their dependents can use this form to access their medical records. |
| Submission Process | Once completed, the form must be submitted to the appropriate military health care facility or office. |
| Privacy Protections | The information provided is protected under the Health Insurance Portability and Accountability Act (HIPAA), ensuring confidentiality. |
| State-Specific Regulations | In some states, additional laws may apply, such as California's Confidentiality of Medical Information Act (CMIA). |
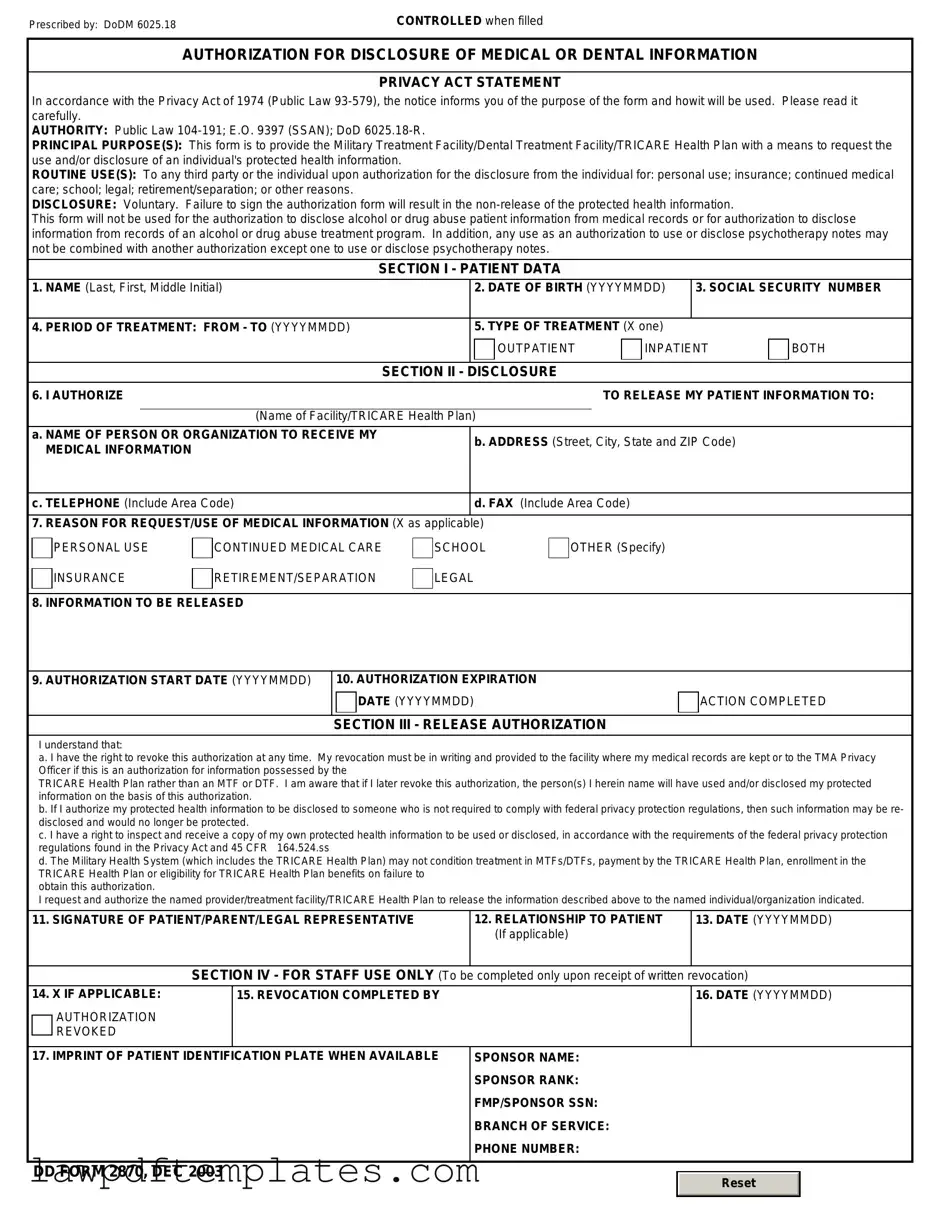
Sample - DD 2870 Form
Prescribed by: DoDM 6025.18 |
CONTROLLED when filled |
AUTHORIZATION FOR DISCLOSURE OF MEDICAL OR DENTAL INFORMATION
PRIVACY ACT STATEMENT
In accordance with the Privacy Act of 1974 (Public Law
AUTHORITY: Public Law
PRINCIPAL PURPOSE(S): This form is to provide the Military Treatment Facility/Dental Treatment Facility/TRICARE Health Plan with a means to request the use and/or disclosure of an individual's protected health information.
ROUTINE USE(S): To any third party or the individual upon authorization for the disclosure from the individual for: personal use; insurance; continued medical care; school; legal; retirement/separation; or other reasons.
DISCLOSURE: Voluntary. Failure to sign the authorization form will result in the
This form will not be used for the authorization to disclose alcohol or drug abuse patient information from medical records or for authorization to disclose information from records of an alcohol or drug abuse treatment program. In addition, any use as an authorization to use or disclose psychotherapy notes may not be combined with another authorization except one to use or disclose psychotherapy notes.
SECTION I - PATIENT DATA
1. NAME (Last, First, Middle Initial) |
|
2. DATE OF BIRTH (YYYYMMDD) |
3. SOCIAL SECURITY NUMBER |
|||
|
|
|
|
|
|
|
4. PERIOD OF TREATMENT: FROM - TO (YYYYMMDD) |
|
5. TYPE OF TREATMENT (X one) |
|
|
||
|
|
|
OUTPATIENT |
INPATIENT |
BOTH |
|
|
|
|
|
|
|
|
|
|
SECTION II - |
DISCLOSURE |
|
|
|
6. I AUTHORIZE |
|
|
TO RELEASE MY PATIENT INFORMATION TO: |
|||
|
|
|
|
|
||
|
(Name of Facility/TRICARE Health Plan) |
|
|
|
||
a. NAME OF PERSON OR ORGANIZATION TO RECEIVE MY |
|
b. ADDRESS (Street, City, State and ZIP Code) |
|
|||
MEDICAL INFORMATION |
|
|
||||
|
|
|
|
|
||
|
|
|
|
|
||
c. TELEPHONE (Include Area Code) |
|
d. FAX (Include Area Code) |
|
|
||
|
|
|
|
|
||
7. REASON FOR REQUEST/USE OF MEDICAL INFORMATION (X as applicable) |
|
|
|
|
||
PERSONAL USE
INSURANCE
CONTINUED MEDICAL CARE
RETIREMENT/SEPARATION
SCHOOL
LEGAL
OTHER (Specify)
8. INFORMATION TO BE RELEASED
9. AUTHORIZATION START DATE (YYYYMMDD)
10. AUTHORIZATION EXPIRATION
DATE (YYYYMMDD)
SECTION III - RELEASE AUTHORIZATION
ACTION COMPLETED
I understand that:
a. I have the right to revoke this authorization at any time. My revocation must be in writing and provided to the facility where my medical records are kept or to the TMA Privacy Officer if this is an authorization for information possessed by the
TRICARE Health Plan rather than an MTF or DTF. I am aware that if I later revoke this authorization, the person(s) I herein name will have used and/or disclosed my protected information on the basis of this authorization.
b. If I authorize my protected health information to be disclosed to someone who is not required to comply with federal privacy protection regulations, then such information may be re- disclosed and would no longer be protected.
c. I have a right to inspect and receive a copy of my own protected health information to be used or disclosed, in accordance with the requirements of the federal privacy protection regulations found in the Privacy Act and 45 CFR 164.524.ss
d. The Military Health System (which includes the TRICARE Health Plan) may not condition treatment in MTFs/DTFs, payment by the TRICARE Health Plan, enrollment in the TRICARE Health Plan or eligibility for TRICARE Health Plan benefits on failure to
obtain this authorization.
I request and authorize the named provider/treatment facility/TRICARE Health Plan to release the information described above to the named individual/organization indicated.
11. SIGNATURE OF PATIENT/PARENT/LEGAL REPRESENTATIVE |
12. RELATIONSHIP TO PATIENT |
13. DATE (YYYYMMDD) |
|
(If applicable) |
|
|
|
|
SECTION IV - FOR STAFF USE ONLY (To be |
completed only upon receipt of written revocation) |
|
14. X IF APPLICABLE:
AUTHORIZATION REVOKED
15. REVOCATION COMPLETED BY
16.DATE (YYYYMMDD)
17. IMPRINT OF PATIENT IDENTIFICATION PLATE WHEN AVAILABLE |
SPONSOR NAME: |
||
|
SPONSOR RANK: |
||
|
FMP/SPONSOR SSN: |
||
|
BRANCH OF SERVICE: |
||
|
PHONE NUMBER: |
||
|
|
|
|
DD FORM 2870, DEC 2003 |
|
|
|
|
Reset |
|
|
|
|
|
|
|
|
|
|
Common mistakes
Filling out the DD 2870 form can be a straightforward process, but many people make common mistakes that can lead to delays or complications. One frequent error is not providing accurate personal information. Double-checking your name, Social Security number, and contact details is essential. A simple typo can cause significant issues down the line.
Another mistake involves misunderstanding the purpose of the form. The DD 2870 is used to request medical records, and it is crucial to specify exactly what records you need. Failing to be clear about the information requested can lead to receiving incomplete records or having your request denied.
Many individuals also overlook the importance of signatures. The form requires a signature from the individual requesting the records. Sometimes, people forget to sign or date the form, which can result in processing delays. Always ensure that your signature is present and that the date is correct.
In addition, some people fail to provide the necessary identification. The DD 2870 may require you to submit a copy of your ID or other supporting documents. Neglecting to include these can lead to rejection of your request. Be sure to review the requirements carefully and include all necessary documentation.
Another common error is not understanding the time limits associated with the request. Some individuals may assume that their request will be processed immediately. However, it can take time for the records to be retrieved and sent. Being patient and allowing for processing time is important.
Many applicants also make the mistake of not keeping copies of their submitted forms. It’s wise to retain a copy of the DD 2870 and any accompanying documents for your records. This can be helpful if you need to follow up on your request later.
Some people fail to follow up after submitting the form. If you do not receive a response within a reasonable timeframe, it’s a good idea to check in. A polite inquiry can help ensure that your request is being processed and that there are no issues.
Another issue arises from not being aware of the fees associated with obtaining records. Some requests may incur costs, and not being prepared for these can lead to unexpected delays. Always inquire about potential fees when submitting your request.
Lastly, individuals sometimes rush through the form without reviewing it thoroughly. Taking the time to read through the entire form and ensuring all sections are complete can prevent mistakes. A careful review can save you time and frustration in the long run.
Common PDF Documents
Tuberculosis Risk Assessment Form - Form completion is a team effort between patient and provider.
For those interested in the rental process, the Georgia Residential Lease Agreement form essentials provide a foundational understanding of the legalities involved in leasing residential properties in Georgia.
Notice of Motion Child Support California - Parents should keep a copy of the completed form for personal records and future reference.