Fillable Advance Beneficiary Notice of Non-coverage Template
File Details
| Fact Name | Description |
|---|---|
| Purpose | The Advance Beneficiary Notice of Non-coverage (ABN) informs Medicare beneficiaries that a service may not be covered by Medicare. |
| When to Use | Healthcare providers must issue an ABN when they believe that a service or item will not be covered by Medicare. |
| Beneficiary Rights | Patients have the right to receive the ABN prior to the service being rendered, allowing them to make informed decisions. |
| State-Specific Forms | Some states may have specific regulations governing the use of ABNs, including additional requirements for notification. |
| Signature Requirement | Beneficiaries must sign the ABN to acknowledge that they understand the potential lack of coverage. |
| Financial Responsibility | If a service is not covered and the ABN was properly issued, beneficiaries may be held financially responsible for the service. |
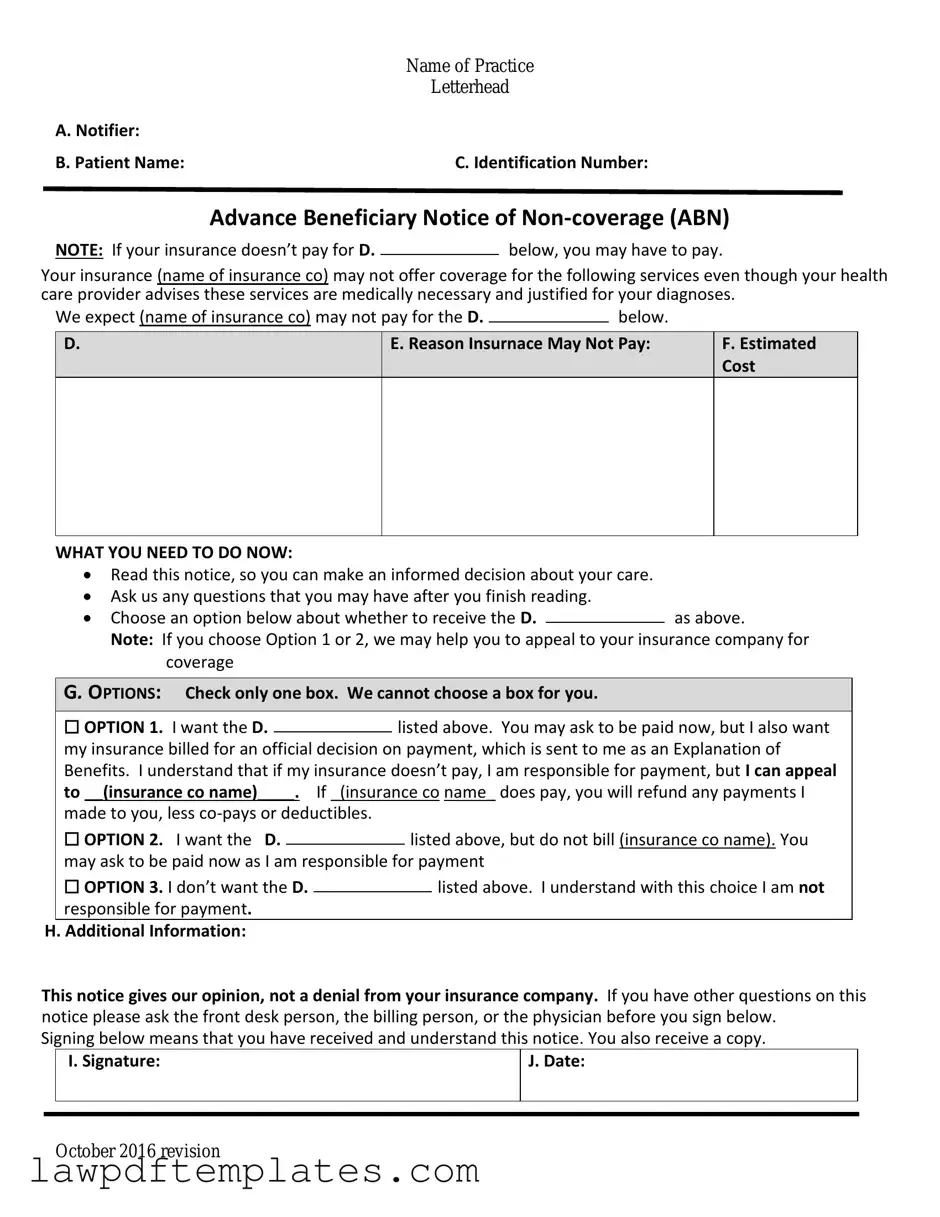
Sample - Advance Beneficiary Notice of Non-coverage Form
|
Name of Practice |
|
Letterhead |
A. Notifier: |
|
B. Patient Name: |
C. Identification Number: |
Advance Beneficiary Notice of
NOTE: If your insurance doesn’t pay for D.below, you may have to pay.
Your insurance (name of insurance co) may not offer coverage for the following services even though your health care provider advises these services are medically necessary and justified for your diagnoses.
We expect (name of insurance co) may not pay for the D. |
|
below. |
|
D.
E. Reason Insurnace May Not Pay:
F.Estimated Cost
WHAT YOU NEED TO DO NOW:
Read this notice, so you can make an informed decision about your care.
Ask us any questions that you may have after you finish reading.
Choose an option below about whether to receive the D.as above.
Note: If you choose Option 1 or 2, we may help you to appeal to your insurance company for coverage
G. OPTIONS: Check only one box. We cannot choose a box for you.
|
☐ OPTION 1. I want the D. |
|
listed above. You may ask to be paid now, but I also want |
||||
|
|
||||||
|
my insurance billed for an official decision on payment, which is sent to me as an Explanation of |
||||||
|
Benefits. I understand that if my insurance doesn’t pay, I am responsible for payment, but I can appeal |
||||||
|
to __(insurance co name)____. If _(insurance co name_ does pay, you will refund any payments I |
||||||
|
made to you, less |
|
|
|
|||
|
☐ OPTION 2. I want the D. |
|
|
listed above, but do not bill (insurance co name). You |
|||
|
|
|
|||||
|
may ask to be paid now as I am responsible for payment |
||||||
|
☐ OPTION 3. I don’t want the D. |
|
|
|
listed above. I understand with this choice I am not |
||
|
|
|
|
||||
|
responsible for payment. |
|
|
|
|||
H. Additional Information: |
|
|
|
||||
This notice gives our opinion, not a denial from your insurance company. If you have other questions on this notice please ask the front desk person, the billing person, or the physician before you sign below.
Signing below means that you have received and understand this notice. You also receive a copy.
|
I. Signature: |
J. Date: |
|
|
|
|
|
|
October 2016 revision
Common mistakes
When filling out the Advance Beneficiary Notice of Non-coverage (ABN) form, individuals often make critical mistakes that can lead to confusion and potential denial of services. One common error is failing to provide accurate patient information. This includes not only the name and Medicare number but also the correct date of service. Inaccuracies can delay processing and create unnecessary complications.
Another frequent mistake is overlooking the explanation of benefits. The ABN requires a clear understanding of why a service may not be covered. If the reason is not articulated properly, it can lead to misunderstandings about the patient's financial responsibility. It's essential to specify the service in question and the rationale for the non-coverage.
Some individuals neglect to sign the form. The signature is crucial as it indicates that the patient understands the implications of the notice. Without a signature, the form may be considered incomplete, which could result in unexpected charges later on. Always ensure that the patient signs and dates the form before submission.
Additionally, people sometimes fail to check the appropriate box regarding their agreement or disagreement with the non-coverage notice. This decision is important for both the patient and the provider. If the wrong box is checked, it can lead to disputes over payment and responsibility for the costs incurred.
Another mistake involves not keeping a copy of the signed ABN for personal records. Patients should always retain a copy for their files. This documentation can be invaluable if questions arise about coverage or billing in the future. Without it, patients may struggle to prove their understanding of the service's coverage status.
Lastly, individuals may not review the form thoroughly before submission. Rushing through the process can lead to overlooked details or errors. Taking the time to carefully review the form can prevent many of these common pitfalls and ensure a smoother experience with Medicare services.
Common PDF Documents
Phone Insurance Claim - This document is tailored for individuals needing help with their electronic devices.
Understanding the importance of the FedEx Release Form can greatly enhance the delivery experience, especially when you're unable to receive a package in person. By utilizing this form, recipients can authorize FedEx to safely leave their parcels at a designated location. For those looking to simplify the process, resources such as Fast PDF Templates offer convenient templates tailored for this purpose, helping to eliminate any potential delivery mishaps.
Texas Temporary Tag - Fill out the form accurately to avoid delays in receiving your tag.
Medication Administration Record Pdf Fillable - Provides a platform for feedback on medication effectiveness.